JIA Subtypes - Overview
Oligoarticular Onset JIA (70% of cases)
Oligoarticular JIA is the most common subtype, typically affecting pre-school girls and often presenting with a single swollen joint, most commonly the knee or ankle. With early recognition and treatment, it generally has the best prognosis.
There is a high risk of chronic anterior uveitis, which is often asymptomatic in the early stages (no pain, redness or visual disturbance). If undetected, this can lead to visual loss due to complications such as cataract or keratopathy. Regular slit-lamp screening is therefore essential.
Blood tests (including rheumatoid factor) and radiographs are often normal. The presence of antinuclear antibodies (ANA) is not diagnostic but indicates an increased risk of uveitis.
Management commonly includes intra-articular corticosteroid injections and physiotherapy. Early treatment helps prevent leg-length discrepancy and muscle wasting. Methotrexate is indicated in children with severe uveitis, involvement of critical joints (e.g. wrist or temporomandibular joint), or those who develop extended oligoarthritis, which occurs in approximately one-third of cases.
The photograph shows swollen ankles in oligo-articular JIA.

The photograph below shows keratopathy as a result of chronic anterior uveitis.

Psoriatic Arthritis
Psoriatic arthritis in children may present as oligoarticular disease, polyarthritis, or an enthesitis-related pattern, and uveitis is relatively common. Skin psoriasis may be absent at presentation, so the diagnosis may rely on associated features such as family history of psoriasis, dactylitis (“sausage digit”), nail pitting, or involvement of the small joints of the hands and feet, often in an asymmetrical distribution.
Management typically includes intra-articular corticosteroid injections and methotrexate, with biologic therapies increasingly used for more severe or refractory disease, particularly where there is significant skin involvement
The photograph shows asymmetrical involvement of the fingers with a restricted distal interphalangeal joint (ring finger) - this is typical of Juvenile Psoriatic Arthritis.

The photograph below shows nail pitting.

The photograph below shows asymmetrical small joint involvement in the hands - asymmetrical small joint involvement is typical in Juvenile Psoriatic Arthritis.

The photograph below shows dactylitis (sausage digit) in psoriatic arthritis.

Enthesitis-Related Arthritis (ERA)
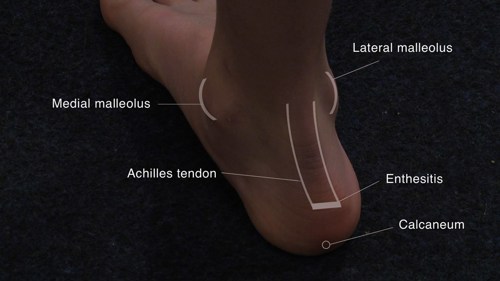
Enthesitis-related arthritis typically affects older boys (over 8 years) and is often associated with HLA-B27 positivity. Children may present with enthesitis and oligoarthritis, most commonly affecting the knees, ankles or hips.
There is overlap with the spondyloarthritis spectrum and with inflammatory bowel disease. Children who are HLA-B27 positive are at increased risk of developing sacroiliitis and axial spine disease in later life, as well as acute anterior uveitis, which presents with a painful red eye (in contrast to the asymptomatic chronic uveitis seen in oligoarticular JIA).
Management includes joint injections and methotrexate for peripheral disease, with biologic therapies increasingly used, particularly where there is axial involvement. Many children with ERA continue to have symptoms into adulthood.
Polyarticular JIA (20% of cases)
Polyarticular JIA typically presents with symmetrical involvement of both small and large joints, most commonly in adolescent girls.
The rheumatoid factor–positive subtype behaves similarly to adult rheumatoid arthritis, with features including erosive disease, rheumatoid nodules and association with HLA-DR4.
Management usually involves early introduction of methotrexate, often given parenterally, and many children require biologic therapy, often in combination with methotrexate, to control disease activity and prevent joint damage.
The photograph below shows polyarthritis affecting small joints of the hands and wrists (Juvenile Idiopathic Arthritis).

The photograph below shows swollen small joints of the hand and a rheumatoid nodule at the elbow.

Systemic Onset JIA (10% of cases)
Systemic JIA is the least common subtype but often the most severe. It typically presents with an acute systemic illness, often in younger children.
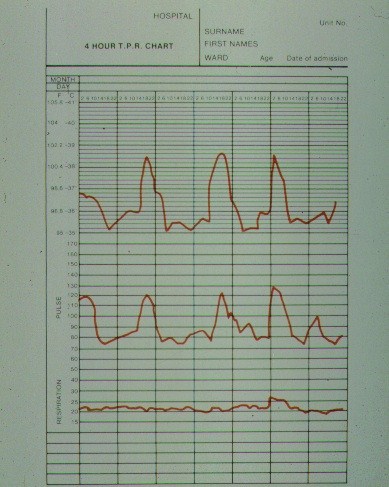
Characteristic features include daily (quotidian) fever spikes, often in the evening; an evanescent maculopapular rash; lymphadenopathy; hepatosplenomegaly; serositis; and markedly raised acute phase reactants and ferritin. The systemic features may precede the arthritis by several weeks.
The differential diagnosis includes infection and malignancy (e.g. leukaemia or neuroblastoma). Complications may include carditis and macrophage activation syndrome, and there is an increased risk of severe infection, particularly in the context of immunosuppressive therapy.
Management requires urgent specialist input and typically includes high-dose systemic corticosteroids (often intravenous in the acute phase), methotrexate, and targeted biologic therapies, particularly IL-1 and IL-6 inhibitors. Refractory cases may be considered for autologous haematopoietic stem-cell transplantation.
The chart below shows the typical fever chart in systemic onset JIA - the fever often occurs in the evening and the rash may appear at times of fever. The fever tends to return to normal in between.