Fever & Arthritis
Poppy is 9 years old and has a 3 week history of pain in her legs and intermittent limp. Blood tests taken by her local doctor were normal. She deteriorated over a weekend with high fever, rash, sore throat and joint pain. She was admitted to her local hospital.
Blood tests showed high acute phase reactants (CRP 200mg/L, ESR 70mm/hr). Throat swab was negative but AntiStreptolysin (ASLO) Titre>400 units. Blood cultures were negative. She was started on IV antibiotics but referred to paediatric rheumatology in view of recurrent fever (often in the evening) with rash. Her joints were normal, there was no splenomegaly but a few small cervical lymph nodes were palpable. Repeat blood tests showed high CRP (120), ESR (98) serum ferritin high (1500ng/L) and anaemia (Hb 8), but blood film normal. Her LDH was high (4000 mg/L).
She was reviewed by haematology and a bone marrow was performed (reactive inflammatory changes only). After several days of antibiotics, she remained unwell with recurrent fever, rash and developed joint pain (hips, knees, hands and wrists, shoulders).
This is Systemic Onset JIA.
- The diagnosis is by exclusion - infection, malignancy to be considered.
- The presentation of SOJIA can be indolent or acute. The arthritis may not be apparent at first but may follow 4-6 weeks after the onset of systemic symptoms.
- Bone marrow may need to be considered to exclude malignancy (leukaemia or neuroblastoma). The peripheral blood film may not show blasts with acute leukaemia.
- It is important to exclude malignancy (leukaemia) before starting corticosteroids as the survival from leukaemia is much worse. It is important to consider a bone marrow if there are atypical features such as a low or normal platelet count (platelets are usually very high with SOJIA), a differential count marrow may need to be considered to exclude malignancy (leukaemia or neuroblastoma). The peripheral blood film may not show blasts with acute leukaemia or where the serum ferritin, is normal or only mildly raised (ferritin, as an acute phase reactant is usually very high in active SOJIA [usually >1000ng/L]).
- In this case the child was unwell, the ferritin was high and there was no apparent arthritis.
Repeat blood tests showed persistently raised acute phase reactants. She was treated with IV corticosteroids, daily over 3 days, improved rapidly and was discharged home on oral steroids to be reviewed after one week. She returned with more joint pain, recurrence of rash and fever. She had polyarthritis.
She was given further course of IV corticosteroids over 3 days and started on subcutaneous methotrexate weekly and discharged on oral steroids to be reviewed for blood tests in 4 weeks.
The family attended weekly to meet the nurse specialist and taught how to administer methotrexate at home. At her 4 week review she was well but had ongoing arthritis, intermittent rash but no fever. She was intolerant of methotrexate, even with antiemetics. After discussion with her family she was started on tocilizumab (IV infusion on the day unit) every fortnight and was able to continue lower dose of subcutaneous methotrexate. After 3 months she was well, in remission and had stopped her steroids. She attends the day unit for infusions of tocilizumab.
The chart shows the typical fever chart - spikes in the evening but normal in between.
A rash may appear at the times of fever. 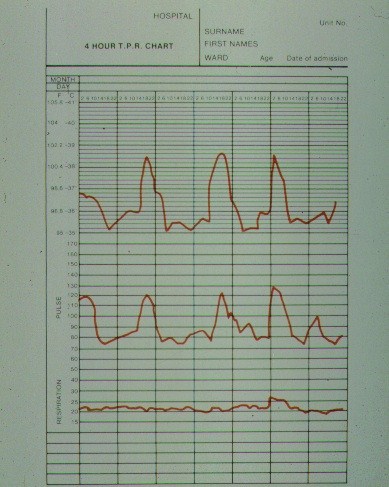
- Tiredness and fatigue; advice about pacing & building up stamina. Family may need support establishing bed times, sleep hygiene & appropriate rest.
- Regular pain relief and anti-inflammatory medication (non-steroid anti-inflammatory drugs NSAIDS) may help relieve joint pain but do not control the disease process.
- Side effects of corticosteroids. Explanation of the need to achieve disease control whilst minimising side effects. Many side effects are reversible; particular support is needed for;
- Weight gain - diet, exercise, consider dietician.
- Methotrexate is often effective but can take several months to achieve disease control.
- With SOJIA, many children require additional treatment with biologics as well as corticosteroids - the latter are tapered and stopped with good disease control from the use of methotrexate with or without biologics.
- NICE guidance is available to inform the use of biologics in JIA.