Bow Legs Knock Knees
Development of the legs in young children involves the following changes:
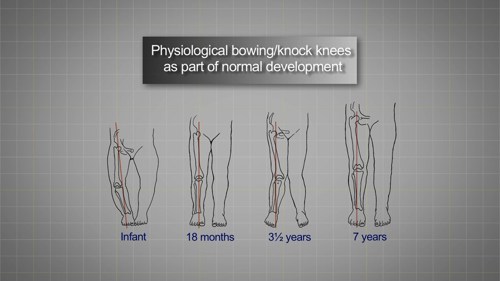
Bow leg (varus) in the infant which aligns to straight legs by 18 months and then into a mild knock knee (valgus) around 3-4 years and straight legs (adult alignment) by around 7 years.
These changes are mild, should be symmetrical and should not cause limp or discomfort.
Bow legs (Genu Varum) are common until 2 years of age.
Referral is necessary if:
- There are signs of asymmetry.
- Changes are associated with pain or functional impairment (e.g., prone to falling).
- Changes are extreme (the femoral intercondylar distance is >6 cm).
- Changes worsen or persist beyond age 4 years.
Conditions to consider include:
Rickets - look for other clinical signs and if relevant, check bone chemistry (calcium, phosphorus and alkaline phosphatase) and vitamin D; especially if the child is failing to thrive, has generalised aches and pains, or has other risk factors such as a vegan diet, malabsorption syndromes or an ‘at risk’ ethnicity.
Skeletal Dysplasias and dwarfism syndromes such as Achondroplasia. It is important to consider growth and limb proportions (short limbs compared to trunk) when suspecting a skeletal dysplasia.
Knock knees are common in young children and most resolve by 6 years of age.
Between the ages of 2 and 4 years, a gap of 6 to 7 cm between the medial malleoli (the bone prominences at the ankles) is common.
Referral is necessary if there is an ankle gap larger than 6-7 cm, pain, asymmetry or if problems persist beyond 5 years of age.
Conditions to exclude are Rickets, Skeletal Dysplasias or Chronic (untreated) Inflammatory Arthritis.