Uveitis
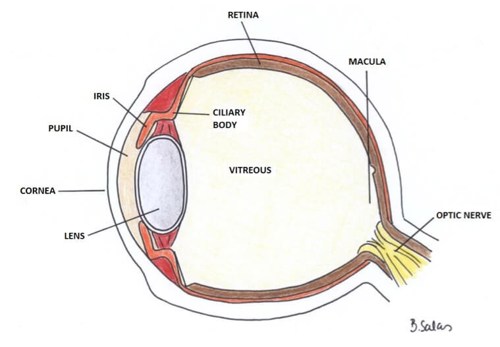
Uveitis refers to inflammation within the eye. This inflammation is mainly within the uveal tract (the vascular layer including the choroid, ciliary body and iris) but can also refer to inflammation of the retina and vitreous.
Uveitis in the iris and ciliary body (the front of the eye) is known as anterior uveitis. If the uveitis is in the ciliary body, then vitreous humour in middle of the eye can be affected (and become cloudy) and this is known as intermediate uveitis. Inflammation in the choroid, involving the retina or retinal vessels, is known as posterior uveitis and can also cause clouding of the vitreous humour.
Juvenile Idiopathic Arthritis (JIA) is the most common systemic disease associated with uveitis in children, affecting around 15% of children with JIA. There are, however, many other causes of uveitis.
In JIA, the typical presentation is chronic anterior uveitis (CAU). This may occur before or after the onset of arthritis, most commonly within the first 7 years of disease.
Importantly, CAU is usually asymptomatic: the eye is not red, there is no pain or photophobia, and vision may initially appear normal. It may be bilateral and is often only detected through routine eye screening. Once symptoms such as blurred vision or floaters develop, the visual outcome is poorer. If undetected and untreated, JIA-associated uveitis can lead to irreversible visual loss or blindness.
Uveitis can occur in any subtype of JIA and at any stage, including before arthritis develops. It is most commonly seen in younger children (under 7 years), those with oligoarticular JIA, and children who are ANA positive.
It is less common in systemic JIA, rheumatoid factor–positive JIA, and enthesitis-related arthritis (ERA). Children with psoriatic arthritis may have an increased risk.
Screening and monitoring
All children with suspected or confirmed JIA should undergo regular eye screening using a slit lamp examination, performed by an ophthalmologist (or an appropriately trained practitioner, depending on local services).
Screening should be carried out at regular intervals and often continues for several years, as uveitis can develop at any time and without symptoms.
Flares may occur during changes or interruption in systemic treatment, and even when arthritis appears inactive.
Poorer visual outcomes are associated with uveitis detected only after symptoms develop and uveitis occurring before arthritis is diagnosed. Visual loss may occur due to complications such as cataract, band keratopathy and glaucoma.
Acute uveitis in HLA-B27–associated disease
Children with HLA-B27–associated JIA (such as those with enthesitis-related arthritis) may develop acute anterior uveitis. This presents differently from chronic uveitis and is typically painful, associated with a red eye, and often photophobic.
This presentation is similar to acute uveitis seen in adults with ankylosing spondylitis. Because acute uveitis is symptomatic, children with ERA and HLA-B27 do not usually require routine screening, as they will present promptly when symptoms occur.
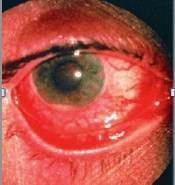
The photograph below shows acute uveitis in HLA B27 related Enthesitis Related Arthritis - the eye is inflamed, painful and photophobic.
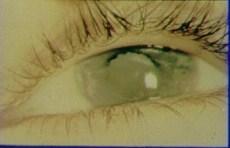
The photograph below shows cataract and keratopathy.