Scoliosis
Scoliosis is a lateral curved deformity of the spine. It is often asymptomatic and may be found incidentally, or may present with symptoms such as back pain. A painful scoliosis is a red flag and referral is needed.
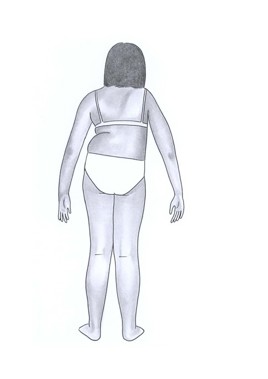
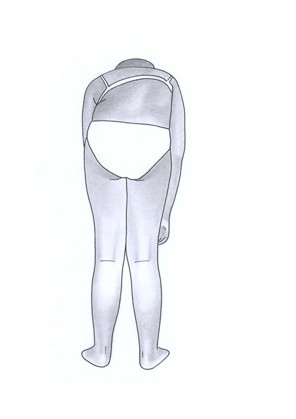
Note the figures below - the graphic on the left showing the asymmetrical skin creases and raised shoulder on one side - these are clues of a scoliosis, which may be more obvious on forward bending (right hand figure).
A structural scoliosis has the most potential of creating cardiovascular or pain problems in later life. Severe scoliosis is likely to cause cardiopulmonary problems.
Acute onset painful scoliosis warrants urgent referral (same day) as serious disease such as infection or malignancy is more likely.
Types of scoliosis are listed below and can result from a spectrum of causes.
Congenital - related to malformation of the vertebra(e), genetic conditions (such as neurofibromatosis or Spina Bifida).
Neuromuscular - related to conditions (such as Cerebral Palsy and Muscular Dystrophy).
Idiopathic - is further divided by age of onset:
- Infantile – onset 0-3 years.
- Juvenile – onset 4-10 years, or before onset of puberty.
- Adolescent – onset over 10 years, or after puberty; >90% of cases of Idiopathic Scoliosis
Management depends on the severity of the curve and age of the child. Bracing and occasionally surgery are needed. Scoliosis present before adolescent growth spurt is more likely to progress.
Other Spinal deformities
The spine in children can be affected by different bone pathologies such as trauma, infection, and tumoral processes. Most typical however are postural deformities, of which the evolution is mainly influenced by growth.
Scheuermann’s 'disease' results from vertebral wedging due to an osteochondrosis of the thoracic spine. This is often asymptomatic (and may be a coincidental finding on radiograph); it can result in thoracic kyphosis, 'slouching appearance', in which case referral to physiotherapy or paediatric orthopaedics is warranted.
Lumbar hyperlordosis is usually physiological and mainly presents around the age of 8 to 10 years, secondary to joint laxity and sometimes slight obesity with a prominent belly. No treatment is necessary since the condition disappears spontaneously.
A thorough history and physical examination are essential because of the high incidence of associated anomalies. Deformities such as scoliosis and hyperkyphosis are best evaluated by imaging - a standing full-spine radiograph followed by Computerised Tomography to study the anatomy of the anomaly and Magnetic Resonance Imaging is important to assess structures including the spinal cord.