Juvenile Idiopathic Arthritis
- Juvenile idiopathic arthritis (JIA) is the commonest cause of chronic arthritis in children in many parts of the world. Juvenile Idiopathic Arthritis (JIA) affects approximately 1 in 1000 children.
- The incidence is 1 in 10,000 per year and prevalence is 1 in 1,000 - this is similar to epilepsy in children.
- The term JIA covers a heterogeneous group of diseases.
- JIA is a diagnosis of exclusion and suspicion of JIA diagnosis rests on careful clinical assessment.
- The differential diagnosis is extensive with conditions ranging from benign (e.g., hypermobility) to life threatening (e.g., malignancy, such as leukaemia and solid tumours, infection, non-accidental injury). The presence of any ‘red flags’, such as weight loss, fever, night pain and bone tenderness warrants urgent assessment with arthritis for six weeks or more, and the cause is unknown (likely a combination of genetic and environmental factors). JIA rarely is familial.
- The definition of JIA is the presence of arthritis for more than six weeks in a child younger than 16 years old and in the absence of other conditions that can cause arthritis.
- The diagnosis of JIA is, therefore, based on the presence and persistence of arthritis and the careful exclusion of any other disease by medical history, physical examination and laboratory tests.
- No laboratory tests, or imaging can ‘prove’ that a child does, or does not, have JIA.
- Laboratory tests for suspected JIA are seldom diagnostic but help to exclude other diagnoses (including malignancy and infection) and are used to monitor disease activity and adverse effects of immunosuppressive drugs.
- Synovial biopsy is not needed to make a diagnosis of JIA. Biopsy is only indicated if there is suspicion of Tuberculosis or malignancy.
- If there is clinical suspicion that a child has JIA, then referral to a paediatric rheumatology team for specialist assessment should NOT be delayed by waiting for tests.
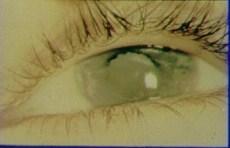
- Time from onset to diagnosis and starting treatment is important - the shorter the interval the better the outcome. In particular, any child suspected of having JIA should be referred for eye screening by slit-lamp examination to detect chronic anterior uveitis (usually without pain or visual symptoms in early stages) and if not detected can result in blindness.
The photograph below shows a blind eye due to cataract and band keratopathy due to chronic uveitis related to JIA
- The clinical assessment of a child is not the same as that of an adult.
- The young child may not be able to verbalise pain and the history may be primarily from the parents or caregivers, or from observations made by teachers and may initially be vague - e.g., 'my child is not quite right' or 'my child is limping'. Examination findings need to be interpreted in the context of normal development.
- The history alone may not localise the site of problems and assessment must include joint examination, as a minimum, pGALS, followed by pREMS of the relevant joints.
- Clues to suggest inflammatory disease:
- Change in behaviour – such as being more irritable, clingy, or reluctant to play.
- Avoidance of activities previously enjoyed (e.g., in play or sport).
- Regression of achieved motor milestones (such as walking or handwriting).
- Morning joint stiffness and pain - the child may be ‘slow to get going in the morning’ or experiences stiffness after periods of rest, such as after long car rides – this is called ‘gelling’.
A detailed approach to the diagnostic work up for suspected JIA is available.