Developmental Dysplasia of the Hip
Developmental Dysplasia of the Hip (DDH), replaces the term Congenital Dislocation of the hip.
There may be a range of severity from acetabular dysplasia, with slight flattening of the acetabulum, to severe dysplasia with abnormal shape of the acetabulum and femoral head. The hip may be stable or unstable, with the potential to sublux and dislocate. DDH affects around 1-3% of all newborns, is more common in girls and 20% are bilateral. Risk factors for DDH include vaginal breech delivery, caesarean breech delivery, oligohydramnios, multiple pregnancy, prematurity, and neuromuscular disorders (e.g., cerebral palsy).
DDH may be detectable at birth, and hence is screened for as part of the newborn check, as well as at the 6 week baby check. This is done by performing Barlow’s and Ortolani’s tests, which examine the ability to dislocate and relocate a femoral head respectively. Limited abduction when the hip is flexed is an important sign - most infants should be able to fully abduct a flexed hip so that the lateral knee touches the examination bed. It is important to assess for asymmetry, but some cases can be bilateral and limited abduction may be present equally on both sides.
When DDH is suspected on screening, diagnosis is confirmed by ultrasound. Babies at high risk are those with a family history of hip problems in early life, breech presentations and should be referred for ultrasound scan of the hips regardless.
DDH may not be detectable or may be missed at birth and some children may present later with limp or hip pain or referred pain to the knee or thigh. After 2-3 months of age, Barlow’s and Ortolani’s tests become more difficult to perform, due to development of muscle tone, and are therefore unsuitable.
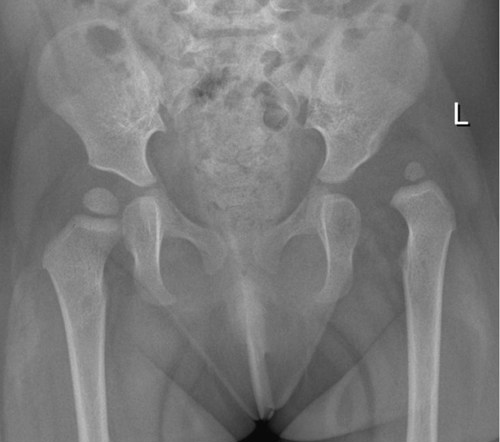
The radiograph below shows DDH at the left hip
After 3 months of age, DDH may be suggested by asymmetrical skin folds, leg length discrepancies, buttock flattening, and walking with the affected leg in external rotation. Older children may present with a gradual onset of a painless limp, tip-toe walking on the affected side, as well as leg length discrepancies.
Early diagnosis is important, as it leads to improved outcomes. The majority of unstable hips in neonates resolve spontaneously within 2-6 weeks, and this can be monitored by ultrasound. Wearing an oversized nappy or diaper helps to keep the hips abducted and femoral head in the acetabulum. If they do not resolve, prompt treatment is required. In children <6 months of age, first line treatment consists of bracing - a harness or splint which must be worn continuously for around 6-8 weeks, being adjusted as the infant grows. The aim is to maintain hip reduction. In children >6 months, splinting and reduction may not be suitable and surgery may be required.
Paediatric Orthopaedic surgeons should be involved in the management of DDH.
Rheumatic fever can present with arthritis of only a single joint; this is a major criterion in the New Zealand ARF diagnostic criteria. Up to a third of children with ARF present with a monoarthritis and of those nearly 80% had carditis confirmed by ECHO. It is however more common for ARF to affect more than one joint and to move from joint to joint. There is usually a prompt response to NSAIDs. This diagnosis should be considered in all those presenting with arthritis with evidence of streptococcal infection and especially in high risk (Maori and Pacific), school-aged populations.