Approach to Suspected JIA
A detailed approach to the diagnostic work up for suspected JIA is available. If there is clinical concern, then referral to paediatric rheumatology for specialist assessment should NOT be delayed - even if blood tests and radiographs are normal and autoantibodies are negative (they can be in JIA!)
The differential diagnosis for JIA is extensive with conditions ranging from the benign to the life threatening red flag conditions (e.g., malignancy, such as leukaemia and solid tumours, infection and Acute Rheumatic Fever).
The pattern of joint involvement is important in the differential diagnosis and also if JIA is confirmed then to determine the JIA subtype. Large joint and intermittent / flitting involvement is typical of Acute Rheumatic Fever and typical patterns of joint involvement in JIA subtypes include:
- Asymmetric, small and large joints, distal interphalangeal joint involvement and dactylitis is typical of psoriatic arthritis (see image below).
- Symmetric, small and large joints is typical of polyarticular JIA.
- Hip involvement, mid-foot (tarsitis) and enthesitis is typical of Enthesitis-Related Arthritis.
- Fever, rash, hepatomegaly, serositis and later symmetrical involvement of small and large joints (including distal small joints of the hands, ankle or wrist involvement) are typical of systemic JIA.
- Investigations are likely to include as a minimum, complete blood count and peripheral smear and Lactate Dehydrogenase to help exclude malignancy), acute phase reactants (Erythrocyte Sedimentation Rate ESR, C-reactive protein CRP, Ferritin), blood chemistry and pending the clinical context, blood cultures or serology for infection (e.g., streptococcal infection).
- ESR and CRP measure the extent of general inflammation, are useful in disease monitoring but can be normal in JIA.
- Ferritin is usually very high in systemic JIA but can also be high in other differentials such as malignancy and infection. Extremely high Ferritin levels associate with Macrophage Activation Syndrome as a complication observed in JIA and other rheumatic diseases.
- Autoantibodies are not diagnostic but are useful.
- The presence of antinuclear antibodies (ANA) in a child with JIA may help identify children at higher risk of developing chronic (asymptomatic) anterior uveitis. ANA are positive in around half the children with oligo-articular JIA.
- However, a small number of normal, healthy children also have a positive ANA, so a positive result does not always mean a child has JIA. SLE must also be considered in the differential diagnosis with a child with joint pain and positive ANA.
- Rheumatoid factor (RF) in the context of JIA is an adverse prognostic factor especially if associated with anti-CCP (cyclic citrullinated peptide) antibodies.
- HLA-B27 is common in many healthy people (5-12%) but is positive in up to 80% of patients with Enthesitis Related Arthritis (ERA).
- In the presence of inflammatory arthritis, HLA-B27 can be associated with axial spine involvement (which may present later on with pain / stiffness in the neck or lower back), sacroiliitis and acute anterior uveitis (which will cause a painful red eye and is different to the chronic anterior uveitis observed in many cases of JIA).
- The presence of HLA-B27 has implications for monitoring and eye screening as it is associated with acute uveitis in ERA. In the context of enthesitis, the presence of HLA-B27 may predict increased likelihood of axial spine involvement (sacroiliitis) which may not be symptomatic until late adolescence / early adulthood.
- Notably HLA-B27 status is not diagnostic and even if negative, with inflammatory back pain, further investigation is needed (i.e., MRI imaging).
- Imaging such as radiographs, ultrasound or MRI may be needed but if the latter is performed, then using gadolinium is very sensitive to detect synovitis.
- MRI of the spine and sacroiliac joints (sometimes with gadolinium) is warranted if the presentation suggests inflammatory back pain as a feature of JIA; radiographs are very difficult to interpret in adolescents and the radiation exposure is considerable.
- Radiographs are useful to assess any damage to the joint, but rarely show any abnormality in early stages of arthritis; they are useful to exclude other causes of joint pain (e.g., trauma / tumour / haematological malignancy). In cases where there is diagnostic difficulty ultrasound or MRI scan may be needed.
- Synovial biopsy is not needed to make a diagnosis of JIA. Biopsy is only indicated if there is suspicion of Tuberculosis (TB) or malignancy.
If there is clinical suspicion that a child has JIA, then referral to a paediatric rheumatology team for specialist assessment should NOT be delayed by waiting for tests. Blood tests and radiographs are initially often normal in JIA, which can provide false reassurance at the time of presentation. The time from onset to diagnosis and starting treatment is important - the shorter the interval the better the outcome. In particular, any child suspected of having JIA should be referred for eye screening by slit-lamp examination to detect chronic anterior uveitis (usually without pain or visual symptoms in early stages) and if not detected can result in blindness.
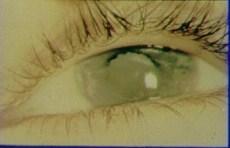
The photograph below shows a blind eye due to cataract and band keratopathy due to chronic uveitis related to JIA
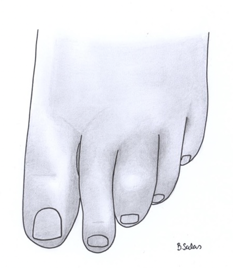
The image below shows a swollen middle toe and tenosynovitis - this is typical of dactylitis in psoriatic JIA.
Further Information
'ThinkJIA' - a resource package to raise awareness about JIA and when to suspect the diagnosis.