Scleroderma
Scleroderma in childhood is rare and there is a spectrum of clinical presentations.
Localized scleroderma is the most common type of scleroderma and can present at any age, with the appearance of a patch (or patches), or linear areas of abnormal skin (called morphoea). Areas of abnormal skin may be red in early phases but are otherwise usually asymptomatic.
- Delay in diagnosis is common as the lesions may be detected coincidentally or considered to be fungal infection or related to trauma. When not treated, morphoea generally follows a course of active expanding disease, fibrosis which can extend deep into subcutaneous tissues resulting in bone (and joint) deformity.
- The functional, cosmetic and psychological impact can be profound. The lesions may interfere with growth of a limb (or foot or hand) or face and skull. Hemi-facial atrophy (Parry Romberg syndrome) and En Coup de Sabre are classical examples of localised scleroderma which can involve deeper tissues; they can be very disfiguring and intracranial lesions can occur.
- Management includes aggressive treatments (corticosteroids and methotrexate, as well as other immunosuppressives) with the aim of limiting severe disfigurement and disability. Further interventions are often needed (e.g., addressing cosmesis and growth abnormalities such as leg length inequality). More information is provided in pmm-nursing.
Systemic scleroderma is extremely rare in children and includes progressive diffuse fibrous changes of the skin and fibrous changes involving internal organs — most commonly lungs, gastrointestinal tract, heart and kidneys — with a significant morbidity and mortality. Raynaud's phenomenon is the most presenting symptom in systemic scleroderma.
- Management: The general approach to management is multi-disciplinary with potent immunosuppression which aims to halt disease activity and organ damage.
The photograph below demonstrates linear scleroderma: the child has a smaller right foot due to chronic disease.

The photograph below shows linear scleroderma with typical 'waxy' pigmented lesions over the foot.

The radiograph below is a barium swallow and shows a dilated oesophagus in systemic sclerosis

The photographs below show tapering of the fingers (sclerodactyly) due to chronic ischaemia and loss of subcutaneous tissues in systemic sclerosis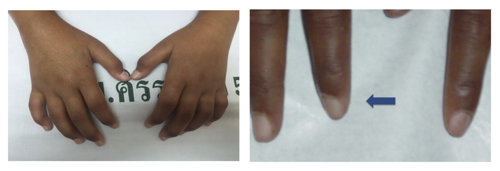
Useful resources to demonstrate skin lesions:
Welcome to Skin Deep - Skin Deep (dftbskindeep.com)
https://www.nottingham.ac.uk/research/groups/cebd/resources/skin-of-colour/index.aspx