In-Toeing
When the foot (or feet) turns inward or outward instead of pointing straight ahead when the child is standing with the legs straight, the foot posture is called, in-toeing (sometimes referred to as ‘pigeon-toeing) or out-toeing respectively. A foot progression angle of up to 10 degrees is normal in children & adolescents (thigh foot angle is explained in pREMS-knee); healthy young children often have a degree of in-toeing which causes no functional impairment and improves with time - in the vast majority resolving by 8-10 years of age.
In-toeing (pigeon-toeing) is common in young children with aetiologies isolating to the hip, below the knee or the feet. Clinical assessment can determine which is the most likely. Most resolve by 10 years of age. Referral guidelines are available.
The three common causes of in-toeing in young children are rotation of the thigh bone (persistent femoral anteversion), rotation of the lower limb below the knee (tibial torsion) and curving of the foot (metatarsus adductus). The changes as a physiological variant are usually symmetrical. Extreme or asymmetrical changes warrant concern and referral for further opinion.
Hips - Persistent Femoral Anteversion - the rotation involves the whole leg and gait observation will show an apparent inward rotation of entire leg. This is common between 3 and 8 years of age and most commonly affects girls more than boys (2:1). The rotation is most obvious when the child is able to sit in a ‘W’ position on the floor
The picture below shows a typical 'W' sitting posture due to Persistent Femoral Anteversion

Lower Leg - Internal Tibial Torsion - the rotation is below the knee. Onset is usually after the child has started walking and usually resolves by 3 years.
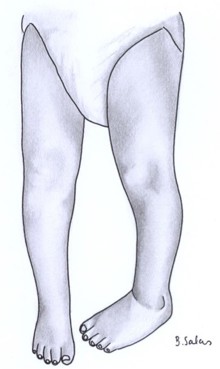
The picture below shows internal tibial torsion (left leg).
Feet - Metatarsus Adductus - the legs are straight but the mid-foot is rotated. Metatarsus adductus improves with age but if persists beyond 6 to 9 months of age and/or is associated with rigid foot, then referral to paediatric orthopaedics is warranted. Serial casting may be of value for the rigid persistent types.
The photo below shows: Metatarsus Adductus with the changes being more obvious on the left - referral is therefore warranted as pathology is more likely.

Indications for referral (to paediatric orthopaedics) for in-toeing:
- Changes are persistent or there is a rigid foot.
- There is pain or a limp or evidence of joint swelling.
- The neurologic examination is abnormal (hypertonia, hyperreflexia, weakness).
- Significant, unilateral disease (possible, but uncommon with benign variants).
- There is associated pain or functional impairment (i.e., child not meeting motor milestones).
- There are functional problems (child clumsy and prone to falling).